New global system to monitor attacks on health care
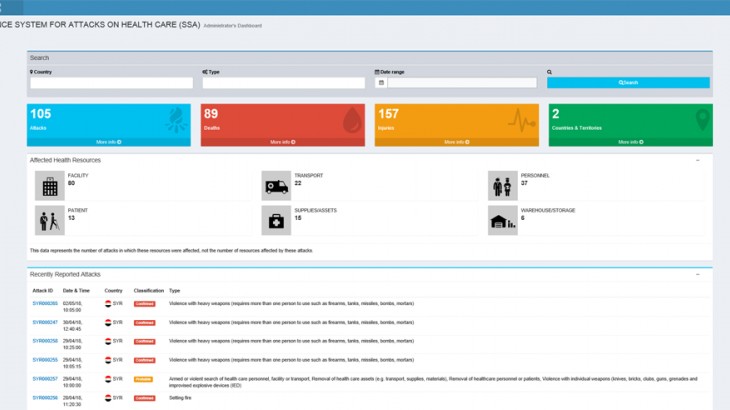
According to a new global surveillance system, 105 attacks on health-care facilities, personnel or resources were reported in the first three months of 2018. With many countries just beginning to submit their data, this number is expected to rise. The online tool, launched by the World Health Organization (WHO) last December, records acts or threats of violence or obstruction that interfere with the availability or delivery of curative and preventive health-care services in conflict- or crisis-affected countries.
To find out more, we spoke to WHO's Carolyn Briody, who was instrumental in setting up the Surveillance System for Attacks on Health Care (SSA).
What is the SSA and who is it designed for?
The SSA collects data on attacks on health care wherever they occur in the world and monitors their impact on the affected population's health, all using a standardized approach.
The tool is aimed at various audiences. These include, of course, health-care personnel and those responsible for the security of health facilities, but also international and national governmental and non-governmental organizations, academics and anyone else interested in this issue.
Through the data collected, we hope to gain a better understanding of the global trends and patterns of this kind of violence, the nature of the attacks, and their repercussions on the delivery of health care. The WHO draws on such information to bolster the current advocacy campaign to end attacks on health care and raise awareness of the relevant rules of international humanitarian law. The ultimate goal is to galvanize action to safeguard health-care services.
Through the data collected, we hope to gain a better understanding of the global trends and patterns of this kind of violence, the nature of the attacks, and their repercussions on the delivery of health care.
Are there other tools available to track violence against health care? If so, what makes the SSA different?
A few other organizations, such as the International Committee of the Red Cross (ICRC), Physicians for Human Rights and the Safeguarding Health in Conflict coalition, collect data on violence against health care. However, their methodologies differ slightly: each has its own definition of what constitutes an attack, so you can't aggregate or compare the information by country. Until now, no global database existed using the same methods and methodology for each country, which is what the SSA does, so results are comparable.
Moreover, it is often difficult, particularly in the heat of a crisis, to confirm the verity of a reported incident; if the criteria are too strict, some incidents, while potentially relevant, may be excluded. For the SSA, epidemiologists therefore developed a grading system with different levels of certainty. Instead of the binary "verified" or "not verified", the SSA has four different levels for each report: (1) rumour, (2) possible, (3) probable and (4) confirmed. All reports graded "possible" and above are published on the "dashboard". Grading is based on the number and reliability of the sources. For instance, an attack suffered or witnessed by a "partner organization", i.e. an organization that is considered by the WHO country office to have reliable information will be graded 4, "confirmed". We include the certainty level of each report on the dashboard. This process allows us to track many more incidents than previous such data-collection systems.
Another advantage of the SSA over other systems is that the data we collect is publicly available: anyone can review both individual incidents and aggregated trends and use them for their own analysis. University students or researchers, for example, might find this useful. We do not publish every single piece of data that we collect, however; any information that is sensitive or might compromise the confidentiality and security of our sources remains private.
Another advantage of the SSA over other systems is that the data we collect is publicly available: anyone can review both individual incidents and aggregated trends and use them for their own analysis.
What are the main challenges and limitations that you have faced so far and how do you see the way forward?
There were quite a few technical and conceptual challenges. I worked closely with our IT experts to find the right balance between the technical aspect and user experience, which took several months.
Such tools rely on a variety of sources. We are actively encouraging existing networks of partners in the Global Health Cluster to report to the system. So far, we have had a good response, in particular from a number of country offices. Our hope is that partners in other clusters, as well as local entities, will also contribute to the system.
For this tool to be effective, and if we are to address the issue of violence against health care more broadly, we need a range of actors – authorities, organizations and individuals – to report cases and promote the system, but also to identify best practices and support measures to protect health care. This is an opportune moment because we already have a coalition of organizations working together to tackle this issue. We are moving in the right direction, but as we can see from the entries in the SSA so far, it is still a major problem, so we must keep up the momentum.
Health Care in Danger is an initiative of the International Red Cross and Red Crescent Movement to make access to, and delivery of, health care safer in armed conflict or other emergencies. This initiative calls for the respect and protection of health care workers, facilities and vehicles and the implementation of a series of recommendations and practical measures to safeguard health care services and their humanitarian mission. This initiative is supported by a number of partners, individuals and organisations, members of the Health Care in Danger Community of Concern.
For more information:
- Visit the Health Care in Danger website
- Join our online community
- Follow @HCIDproject on Twitter and join our call to #protecthealthcare
- Sign up to our newsletter and stay informed